Diseases and conditions contributing to NCD premature mortality
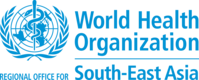
Policy-makers could consider the relative burden of disease in their prioritization exercise. Some conditions will be more important in a particular country than in others. Fig. 6 provides rankings of specific NCD causes in the South-East Asia Region Member States (37). While cardiovascular diseases are top causes of NCD mortality in some countries, other conditions may warrant special consideration. The numbers in this figure show the rank of each specific cause as a contributor to overall mortality from NCDs in 2019. The colours show the historical annual rates of change (2015–2019) for each cause. Meeting the SDG 3.4 target requires at least a 2.7% annual rate of decline in mortality from each NCD. The light and dark blue colours imply that a country is on track to achieving the target for that cause, and the yellow, orange, and red colours imply that a country is off track. Conditions listed are indicative, and grouping them as the four major NCD categories may change the order. The main purpose is to consider such analysis with detailed national data.
Fig. 6. Ranking and yearly percentage change in cause-specific probability of dying
| SEAR | BAN | BHU | IND | INO | MAL | MMR | NEP | DPR Korea | SRL | THA | TLS | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ischaemic heart disease | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 1 | 2 | 1 |
| Chronic respiratory disease | 2 | 4 | 2 | 2 | 4 | 6 | 4 | 1 | 3 | 3 | 8 | 3 |
| Hamorrhagic stroke | 3 | 2 | 3 | 3 | 2 | 3 | 1 | 3 | 1 | 5 | 5 | 2 |
| Diabetes | 4 | 5 | 5 | 4 | 3 | 2 | 3 | 6 | 8 | 2 | 4 | 4 |
| All other cardiovascular diseases | 5 | 6 | 6 | 5 | 6 | 10 | 7 | 4 | 6 | 6 | 13 | 5 |
| Upper aerodigestive tract cancers | 6 | 3 | 7 | 6 | 9 | 9 | 6 | 8 | 11 | 4 | 6 | 8 |
| Ischaemic stroke | 7 | 7 | 10 | 7 | 5 | 12 | 5 | 9 | 5 | 9 | 10 | 6 |
| Lung cancer | 8 | 8 | 8 | 9 | 7 | 4 | 8 | 7 | 4 | 7 | 3 | 7 |
| Breast cancer | 9 | 10 | 14 | 8 | 8 | 5 | 12 | 10 | 13 | 8 | 9 | 11 |
| Stomach cancer | 10 | 9 | 4 | 10 | 14 | 14 | 10 | 11 | 9 | 10 | 14 | 14 |
| Colon and rectum cancers | 11 | 12 | 12 | 11 | 12 | 11 | 13 | 13 | 10 | 13 | 7 | 10 |
| Cervix uteri cancer | 12 | 11 | 9 | 13 | 10 | 8 | 11 | 5 | 14 | 14 | 12 | 13 |
| Liver cancer | 13 | 14 | 11 | 14 | 11 | 7 | 9 | 14 | 7 | 11 | 1 | 9 |
| All other cancers | 14 | 13 | 13 | 12 | 13 | 13 | 14 | 12 | 12 | 12 | 11 | 12 |
Source: NCD Countdown 2030 Collaborators (37)
yearly percentage change in cause-specific probability of dying

South-East Asia Region NCD impact simulation tool
The South-East Asia Region NCD impact simulation tool (40) has been developed to assist Member States in the region prioritize different NCD interventions for their national NCD response (41). The tool uses the intervention list, modelling approach and data inputs from NCD Countdown 2030 (42). Various tabs in the tool guide the user through the process of reviewing data inputs, specifying key parameters (e.g. baseline and target coverage) and visualizing results. The tool is meant to be an input to the policy dialogue process, not a prescription for specific actions. It is not meant to supplant the expertise of various technical working groups or units (e.g. departments of planning) within ministries of health. The tool includes estimates of the unit cost to the health system of each intervention, taken from the literature. These unit cost estimates can be replaced with local data, e.g. from primary micro-costing studies or OneHealth Tool costing spreadsheets. Care should be taken to align the local cost data with the descriptions of the interventions. The tool uses the population model described previously to provide projections of costs between 2023 and 2030, including “incremental costs” (i.e. additional costs required to scale up the interventions) and “total costs” (i.e. current spending plus incremental costs).
In addition to the current and target coverage levels of each intervention, which impact the incremental and total costs, the tool also includes a parameter specifying the current and target share of out-of-pocket costs for each intervention. Efforts to reduce out-of-pocket costs, especially for interventions in the high-priority category, will be reflected in the incremental and total costs above and beyond the costs of simply scaling up the interventions at their current levels of out-of-pocket spending.
Achieving the SDG 3.4 target will require countries to scale up interventions faster than has been observed historically. The tool includes a parameter for each intervention that specifies the rate of increase in population coverage of each intervention. The default coverage increase is set as an annual 2% increase on the 2022 coverage, resulting in an increase of 16% by 2030. For reference, most low- and middle-income countries have had increases in hypertension treatment coverage of less than 1% per year; the best-performing countries have had increases of just under 2% per year. Coverage of antiretroviral drug therapy has typically increased at between 4% and 5% per year, and represents an upper limit of what is logistically feasible during the SDG period until 2030. The choice of scale-up rate has a direct impact on the likelihood of achieving the SDG 3.4 target: the faster the increase in coverage, the greater the benefits of the intervention on population mortality, but at higher incremental cost.